Have you ever gotten up in the morning, rolled out of bed, and all of a sudden felt like the entire room was spinning around you? Or perhaps you glanced up at a shelf, and the world tipped sideways for a couple of horrifying seconds? This spinning sensation, especially when triggered by a simple head movement, has a name. It is known as BPPV or Benign Paroxysmal Positional Vertigo.
The good news? BPPV is not harmful. The even greater news? It is often regarded as a one-time, clinic-based treatment. So now, we will break it down into simple terms: what it is, why it happens, and, above all, how we can get rid of it as quickly as possible.
What Is Benign Paroxysmal Positional Vertigo and Why Is It So Common?
One of the most common causes of vertigo worldwide is Benign Paroxysmal Positional Vertigo. Indeed, it is estimated to account for virtually half of all vertigo cases observed in balance clinics.
Let’s break down the name:
- Benign: it is not life-threatening.
- Paroxysmal: it is sudden and short-lived.
- Positional: It is triggered by changes in head position.
- Vertigo: the sensation of spinning.
So, when someone says they only feel dizzy when they turn over in bed, bend down to pick something up, or tilt their head back, then there is a very good possibility that they are dealing with benign paroxysmal positional vertigo.
Know More About
- BPPV in Elderly Patients: Why Age Changes Treatment Approach
- BPPV vs Persistent Postural-Perceptual Dizziness (PPPD): Key Differences
- How Do I Know If My Vertigo Is BPPV or Something Else?
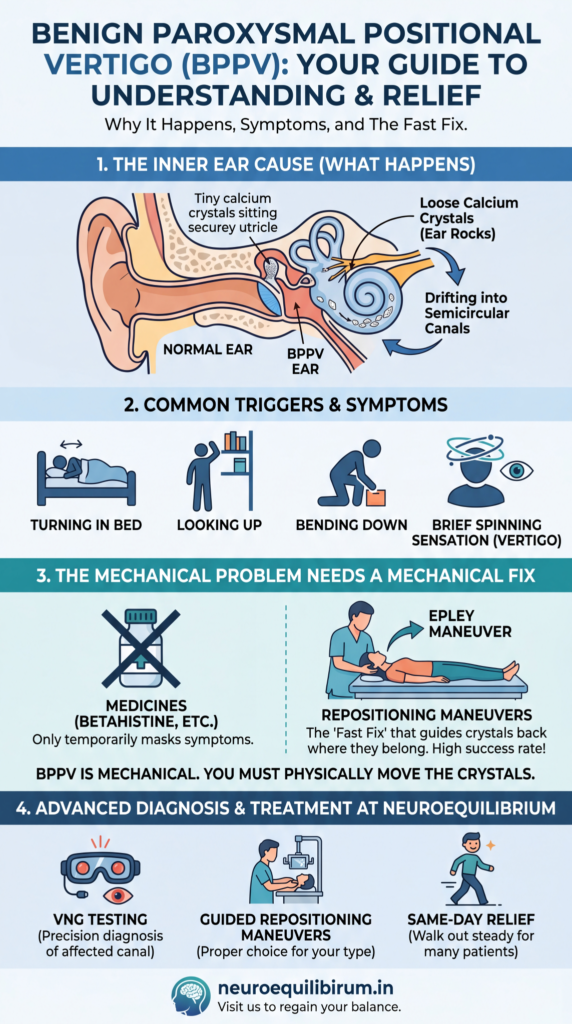
What Really Happens Inside Your Ear When BPPV Strikes
Inside your inner ear is a tiny but complex balance system that informs your brain of where your head is in space. Within this system, there is a tiny organ known as the utricle, which contains microscopic calcium crystals (called otoliths or ear rocks) that help you feel the effects of gravity and movement.
In benign paroxysmal positional vertigo, these crystals become dislodged from their usual place in the utricle and accidentally drift into the fluid-filled semicircular canals, the tube-shaped parts of the inner ear that detect rotational movement.
And, as you turn your head, “these displaced crystals move inside the canal and disturb the fluid, pushing the fluid in the opposite direction. This gives a false alarm to your brain, and it makes it think your body is spinning around like a top, even when you are lying motionless. That is the spinning sensation you experience. This is BPPV at work.
Why Do These Crystals Fall Out of Place? Common BPPV Causes Explained
Benign paroxysmal positional vertigo does not necessarily have a clear cause, but a number of known triggers can dislodge the ear crystals:
- Head injury or trauma: Even a mild bump to the head can cause the crystals to be knocked out.
- Aging: BPPV is particularly prevalent in adults older than 65 years, as the crystals naturally become less stable with age.
- Long-lasting bed rest: Spending too much time in one position, such as after surgery or during illness, can lead to crystal migration.
- Prolonged or unusual head positions: Keeping the head in one position for extended periods, such as in a dentist’s chair or during a salon hair wash, may contribute.
- Inner ear infections or migraines: Underlying conditions like vestibular migraine or labyrinthitis can increase the risk of BPPV.
- Vitamin D deficiency: Some studies have linked low Vitamin D levels to an increased risk of crystal displacement and BPPV recurrence.
- Spontaneous occurrence: Very often, benign paroxysmal positional vertigo can occur on its own with no apparent cause whatsoever.
A 2024 PMC research confirms this link: A randomized trial found BPPV patients had significantly lower Vitamin D levels, with deficiency in 71% of cases, increasing recurrence risk. Supplementation reduced episodes by 60%.
How Long Does a BPPV Episode Last, and What Does It Feel Like?
The typical duration of a classic benign paroxysmal positional vertigo episode is less than one minute, usually between 10 and 30 seconds. Even though it is brief, those few seconds can feel frightening.
Common symptoms include:
- A sudden spinning sensation when changing head position.
- Feeling as if the room is moving even though you are still.
- A brief wave of nausea or the urge to vomit.
- Unsteadiness or loss of balance immediately after the spinning.
- Uncontrolled eye movements, known as nystagmus.
One important thing to note: BPPV vertigo is always provoked by motion. When the room itself starts spinning even when you are sitting perfectly still and not moving your head at all, that may indicate an alternative type of vestibular disorder, and a proper diagnosis becomes even more critical.
Why Benign Paroxysmal Positional Vertigo Cannot Be Cured With Medicines Alone
This is among the most important things to be aware of about BPPV. Some individuals go to see a doctor, are prescribed anti-vertigo medication, and wait until things improve. However, the spinning continues to recur because medication cannot correct the underlying mechanical issue.
Benign paroxysmal positional vertigo is a mechanical problem. The crystals are literally out of place. No pill can move them back into place. Medicines such as betahistine, meclizine, etc may temporarily reduce dizziness symptoms, but they do not treat the underlying cause.
Think of it like a tiny pebble lodged in a pipe. Medicine will do no good in opening the pipe; you must use the proper method of forcing the pebble out.
The Fast Fix: Repositioning Maneuvers That Can Treat BPPV in Minutes
The true treatment of benign paroxysmal positional vertigo is a series of specific guided head-and-body motions known as repositioning maneuvers. They are performed by trained specialists and are intended to physically guide displaced crystals out of the semicircular canals and back into the utricle, where they belong.
The best-known and most commonly used of all types of BPPV is the Epley Maneuver, used to treat the most common type of BPPV, posterior canal BPPV. It has an 80-90% success rate and takes only a few minutes to complete.
But here is something most people do not know: there are several variants of BPPV, depending on which canal the crystals have entered and how they move within it. This means one maneuver may not work for every case. Since each diagnosis is different, the Semont maneuver, the Barbecue Roll, the Gufoni maneuver, or another specialized technique may be used to treat the exact type and location of crystal displacement.
Choosing the wrong maneuver for the canal involved can worsen symptoms; as such, it is absolutely essential that a proper diagnosis be made before treatment is administered.
“Correct diagnosis guides the selection of the correct maneuver. This non-invasive maneuver can be performed on the same day. It’s almost magical to see how a patient enters the clinic with dizziness and exits more stable and confident.
We get patients who have been admitted to the ICU; some come on a stretcher. But after correct diagnosis followed by the therapeutic maneuver, patients can go back home walking with a smile on their face.”
Dr. Anita Bhandari, Co-founder, NeuroEquilibrium Vertigo Clinics
How Specialists Diagnose the Exact Type of BPPV Using Advanced Testing
To perform the correct maneuver, a specialist must first identify which canal the crystals are lodged in. This is done through positional tests such as the Dix-Hallpike test or the Supine Roll Test, while the specialist closely observes the patient’s eye movements.
The involuntary flickering eye movements, called nystagmus, help a trained specialist identify which ear and which canal are affected, and which particular form of benign paroxysmal positional vertigo the patient has.
In advanced balance clinics, a technology called Videonystagmography (VNG) uses high-speed infrared cameras to precisely track and record nystagmus movements. This eliminates guesswork and makes the diagnosis much more precise. Once the affected canal is identified, the appropriate maneuver is performed, and patients tend to walk out feeling greatly improved on the very same day.
This is not a far-fetched thing. Once BPPV is properly diagnosed and the correct maneuver is performed, the recovery can seem almost instant.

Why Choose NeuroEquilibrium for BPPV Diagnosis and Treatment?
Successful treatment of benign paroxysmal positional vertigo depends heavily on an accurate diagnosis, which may not always be available in general clinics.
NeuroEquilibrium is the largest chain of vertigo and balance disorder clinics in India, has one purpose: to diagnose and treat vertigo and balance disorders effectively. Here is what makes the approach different:
- Specialized VNG Testing: High-speed infrared cameras capture your nystagmus patterns and help ensure that the specific form of benign paroxysmal positional vertigo is accurately identified.
- BPPV Maneuver Guidance System: This proprietary, technology-assisted system helps specialists select and perform the most suitable repositioning maneuver for your case.
- Thorough Vestibular Assessment: Tests such as the Video Head Impulse Test (vHIT), Computerized Posturography, and Rotary Chair examination help rule out other balance disorders and reduce the risk of misdiagnosis.
- Same-Day Relief: When the diagnosis and maneuver are correct, most BPPV patients experience significant relief during their very first visit.
- Online Rehabilitation: Virtual vestibular rehabilitation programs can be used to provide home-based recovery.
If you or a loved one has been experiencing unexplained spinning, dizziness, or balance problems triggered by head movements. NeuroEquilibrium specializes in exactly that, and the path to feeling steady again may be shorter than you think.
Summary in a Nutshell: What You Need to Know About Benign Paroxysmal Positional Vertigo
The most frequent cause of vertigo is benign paroxysmal positional vertigo, a condition caused by displaced calcium crystals in the inner ear.
- It causes brief but intense spinning triggered by certain head movements.
- It usually cannot be corrected with medicines alone; repositioning maneuvers are the main treatment.
- BPPV has different variants, so accurate diagnosis is important before treatment.
- Most patients can feel better that very day, with the right specialist and the right maneuver.
- High-quality diagnostic instruments, such as VNG, enable rapid and accurate diagnosis.
If the room spins every time you roll over in bed, your inner ear may be asking for help. Contact a specialized balance clinic and find the right solution quickly.
How do you prevent BPPV attacks?
To reduce attacks of Benign Paroxysmal Positional Vertigo, avoid sudden head movements, get up slowly from bed, use extra pillows if lying flat triggers symptoms, stay hydrated, and manage stress or sleep deprivation that can worsen dizziness. Vestibular exercises and corrective repositioning maneuvers for recurrent inner ear crystal displacement can also reduce recurrence.
How long does benign paroxysmal positional vertigo last?
A spinning episode from Benign Paroxysmal Positional Vertigo usually lasts only a few seconds to one minute after a position change, but the condition itself can continue causing repeated episodes for days or weeks if untreated. With proper repositioning treatment, many people improve much faster.
What triggers benign paroxysmal positional vertigo?
Benign Paroxysmal Positional Vertigo is commonly triggered by turning over in bed, looking up, bending down, sudden neck movements, head injury, prolonged bed rest, or age-related inner ear changes. These movements shift loose calcium crystals inside the balance canals and provoke spinning.
How do you fix benign positional vertigo?
The Epley Maneuver or various Otolith repositioning procedures are the best method of treating Benign Paroxysmal Positional Vertigo. These motorized head movements are used to move the displaced crystals back to the appropriate chamber of the inner ear (utricle), often resulting in symptom relief without medication.
What vitamin am I lacking if I get vertigo?
Low vitamin D levels may be associated with reduced calcium metabolism in the inner ear and with the recurrence of vertigo in some people. In some cases, deficiencies in vitamin B12 or iron can also cause dizziness; therefore, persistent symptoms may indicate a vitamin D3,vitamin B12 or iron deficiency.